
A basic article for understanding hypomania.
The state where you feel awesome, yet act counterproductively.

It’s George.
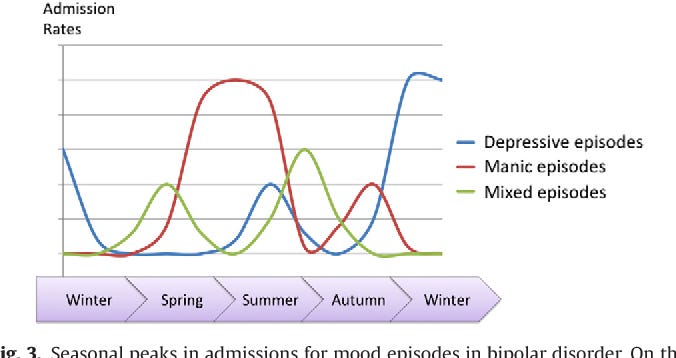
Hypomanic and manic episodes are beginning to peak this season so i thought that i should write a quick article about hypomania.
But as always, listen to your doctor. Nothing in this article should be viewed as a substitute for medical advice.
Now hypomania is a distinct mood state involving abnormally and persistently elevated, expansive, or irritable mood accompanied by increased energy or activity.
It is milder than full mania and does not cause the same level of severe impairment, psychosis, or need for hospitalization.
According to the DSM-5-TR, a hypomanic episode requires all of the following:
Criterion A: A distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy. This must last at least 4 consecutive days, present most of the day, nearly every day.
Criterion B: During this period, at least 3 of the following symptoms (4 if the mood is only irritable) must be present to a significant degree.
They must represent a noticeable change from the person’s usual behavior:
Inflated self-esteem or grandiosity.
Decreased need for sleep (feeling rested after only 3 hours).
More talkative than usual or pressure to keep talking.
Flight of ideas or subjective experience where thoughts are racing.
Distractibility (as reported or observed).
Increase in goal-directed activity (socially, at work/school, or sexually) or psychomotor agitation.
Excessive involvement in activities that have a high potential for painful consequences (the typical ones are unrestrained buying sprees and hypersexuality).
Criterion C: The episode is associated with an unequivocal change in functioning that is uncharacteristic of the individual when not symptomatic.
Criterion D: The disturbance in mood and change in functioning are observable by others.
Criterion E: The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization.
So there are no psychotic features such as delusions or even hallucinations present.
Criterion F (and a quite important one): The symptoms are NOT attributable to the direct physiological effects of a substance or another medical condition.
If you choose for example to do modafinil, tren, T3, sabroxy, rhodiola and 400mg of caffeine, you do not have bipolar. You are <redacted>.
I can not stress this enough.
The amount of stimulants a lot of people consume are enough to put a lot of mentally healthy people in a borderline hypomanic state.
Now hypomania has some key distinctions from mania such as its:
Duration: Hypomania lasts ≥4 days while mania lasts ≥7 days.
Severity: Hypomania does not cause marked functional impairment or psychosis while mania does and often leads to hospitalization.
Experience: People in hypomania often feel productive, creative, or euphoric and may function well (or even better than usual) in the short term, though poor judgment can still lead to consequences.
Hypomania is often noticeable to others but may feel subjectively positive to the individual.
Now it is a core feature of several mood disorders but can also appear secondarily in other psychiatric, medical, neurological, or substance-related conditions.
Here is a comprehensive list based on clinical literature (BUT, i could be missing something, so let me know if this is the case):
Bipolar II disorder
Cyclothymic disorder/Cyclothymia (it’s still labeled as BD-III in some textbooks)
Bipolar I disorder
Now of course, do not self-diagnose yourself with it because emotional dysregulation can mimic or co-occur with hypomanic-like states for example.
So if you have severe ADHD for example, you can 100% mislabel what’s going on during certain periods as hypomania.
Now hypomania arises from a complex, multifactorial interplay of genetic vulnerability, neurobiological factors (think brain circuits and neurotransmitter systems), environmental triggers and lifestyle influences that disrupt the brain’s ability to regulate mood, energy, reward, and arousal.
We’ll talk about all of them.
First and foremost, even though no single gene causes hypomania (or bipolar, or ADHD, or this or that (everything usually is polygenic)), when it comes to the links between genetic variants and pathophysiological mechanisms in hypomania, one of the most consistently replicated is in the CACNA1C gene.
This gene encodes the alpha-1C subunit of L-type voltage-gated calcium channels (Cav1.2).
These channels control calcium influx into neurons, which influences:
Neuronal excitability
Neurotransmitter release (especially glutamate and dopamine)
Gene expression
Synaptic plasticity (the brain’s ability to strengthen or weaken connections)
The risk allele rs1006737 (A allele) is one of the strongest and most replicated associations with hypomania and bipolar disorder.
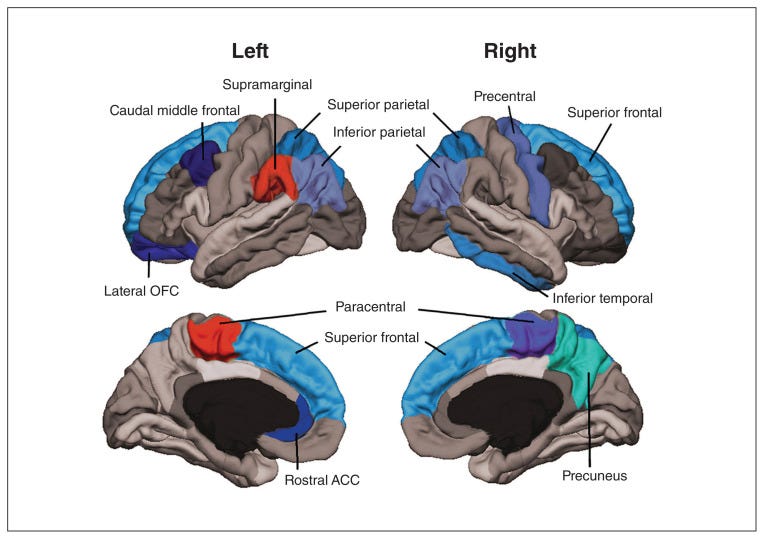
It has been linked to altered brain structure (reduced cortical thickness in prefrontal and parietal regions), changes in functional connectivity, and differences in cognitive performance (such as working memory and attention).
Other notable genes include ANK3.
This gene encodes a protein that anchors voltage-gated sodium channels at key points in neurons (the axon initial segment).
It is critical for:
Action potential generation
Neuronal signaling
Maintaining proper excitability
Variants in ANK3 such as rs1099433, are also strongly associated with hypomania and bipolar disorder and can affect cognitive functions like attention and memory.
Other notable genes and pathways can include:
Variants affecting circadian rhythm genes.
Genes involved in neurotransmitter systems (anything that affects dopamine, serotonin, glutamate signaling, whether that’s called SNPs in COMT or MAO).
Heck, even anything that can lead to elevated NE turnover can have a big effect.
Genes related to neurodevelopment and synaptic function such as ODZ4, DGKH, NCAN in some GWAS.
But overall, the highest risk comes with issues in CACNA1C and ANK3.
This of course does not mean that you are hopeless against your genetics.
What it means is that you need to prioritize monitoring certain environmental factors better.
I have a friend for example who has type II bipolar and is doing fine.
In fact, if you talked to him, you wouldn’t even guess that this might even be the case.
So you can usually manage these issues with the right tools/roadmap.
Now let’s talk a bit about brain chemistry and neurobiology.
There is dysregulation in multiple neurotransmitter systems and interconnected brain circuits during hypomania.
How else could you expect to experience heightened energy, euphoria/reward sensitivity, racing thoughts, and impulsivity?
There are a lot of things going on simultaneously and these changes are not simple “excess” or “deficiency” of one chemical but rather dynamic imbalances that shift with mood states.
Think that in hypomania, the brain often operates in a “revved-up” mode with reduced regulatory control.
The central role in this of course, has dopamine.
Its surges, particularly in the mesolimbic pathway heighten incentive salience and reward sensitivity.
This creates the classic “everything feels possible”, “everything is awesome (ideas etc)” sensation, increased goal-directed activity, talkativeness, higher libido and euphoria.
While this dopamine boost can feel highly productive in the short term, it also reduces the brain’s ability to weigh long-term consequences, contributing to risk-taking behaviors and very impulsive decisions.
The impact of serotonin is also quite interesting with fluctuations or altered receptor function being mplicated with changes in turnover contributing to the elevated or unstable mood in hypomania.
Norepinephrine is of course, the king of the “wired but not tired” that starts kicking in after a couple of days.
It enhances global brain activation via widespread projections to the prefrontal cortex, amygdala, hippocampus, and other regions.
This creates a state of heightened vigilance and mental sharpness, making the person feel “wired” and ready for action even without external stimulation.
Elevated norepinephrine promotes wakefulness by stimulating the reticular activating system and interacting with other arousal-promoting systems (such as the orexin/hypocretin (we’ve talked about all these in previous articles https://healthlibrary.substack.com/archive) and it also amplifies the fight-or-flight response, increases heart rate, blood pressure, and psychomotor activity.
Now glutamate is the brain’s primary excitatory neurotransmitter, responsible for the majority of fast synaptic transmission and playing a critical role in learning, memory, synaptic plasticity, and overall neuronal communication.
In hypomania (and manic states), research consistently points to increased glutamatergic signaling and heightened activity at NMDA receptors.
NMDA receptors are ionotropic glutamate receptors that, when over-activated, allow excessive calcium influx into neurons.
This triggers cascades that increase neuronal firing rates, promote excitotoxicity (over-stimulation that can damage cells if prolonged), and enhance synaptic strength in an uncontrolled way.
In hypomania, this heightened excitability is thought to drive:
Racing thoughts and flight of ideas: Rapid, uncontrolled spread of neural activation across cortical networks.
Heightened energy and arousal: Amplified excitatory drive across motor and motivational circuits.
Emotional intensity and lability: Stronger emotional tagging of experiences and quicker shifts in reactivity.
Impulsivity and reduced sleep need: Overriding normal regulatory mechanisms that promote rest and behavioral inhibition.
This creates a state of cerebral hyper-excitability, sometimes described metaphorically as the brain’s “accelerator” being pressed too hard without adequate “brakes” (from GABA or prefrontal regulation).
Some researchers link this to increased glutaminolysis and hyperglycolysis — metabolic shifts that provide extra energy for this heightened activity during manic/hypomanic states.
Side note: If the theory that BD is driven by "overactive" PC holds true, excess biotin could theoretically increase brain glutamate levels, potentially contributing to the glutamatergic hyperactivity seen in manic phases which is another reason to not use doses higher than 300mcg for no real reason.
Also keep in mind that valproate can interfere with biotin metabolism and carbamazepine can lower serum biotin levels by up to 50%.